
All of us misplace keys, forget people’s names and phone numbers or forget where we parked the car/bike. When this happens while we are young, we seldom believe it is a problem. However, as we age we are prone to worry that these events may be a sign of impending dementia or Alzheimer’s disease.
Dr. Niyom Pisitpipattana, M.D., a neurologist from Bangkok Hospital Pattaya helped his Pattaya City Expats Club audience at their August 20 meeting to understand what is normal, what’s not and when to seek help.
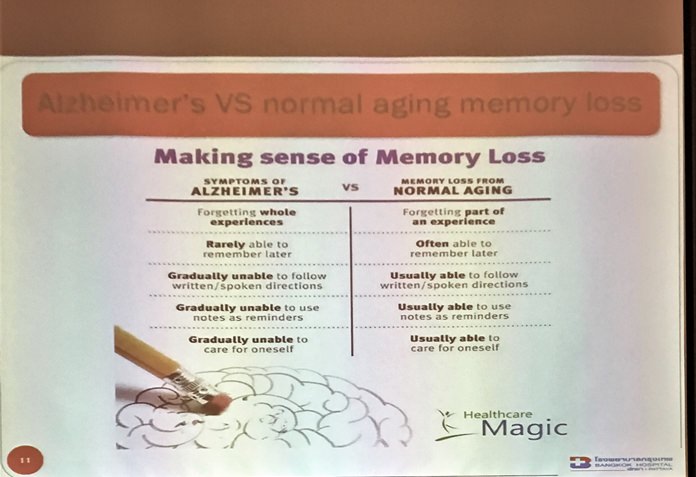
He mentioned that memory lapses are often frustrating, but most of the time, they should not be a cause for concern. Further, age-related memory changes are not the same thing as dementia. As we grow older, we experience physiological changes that can cause glitches in brain functions, which is well recognized. It takes longer to learn and recall information and we are not as quick as we used to be. In fact, we often mistake this slowing of our mental processes for true memory loss. But in most cases, if we give ourselves time, the information will come to mind.
He explained that memory is simply the ability of the brain to learn or remember new information, place that information in certain compartments of the brain, then recall the information when needed. Memory function problems can be caused by factors not related to dementia or Alzheimer’s disease and may be treatable. For example he cited injury, stress, lack of sleep, substance abuse, depression or metabolic disorders can cause memory loss which may be temporary/treatable. Thus, symptoms of memory function problems require careful medical evaluation.
Mild Cognitive Impairment (MCI) is a stage between normal age-related issues and the more serious onset of dementia. This stage is not always clearly defined and is often just a matter of the degree of the issues. For example, it is normal as you age to forget a person’s name; however, it is not normal to forget the name of close family members or friends, even after a period of time. Family members or close friends will likely be aware of the condition, but your ability to function in your daily life means that you do not necessarily have dementia. Some people with MCI plateau at a relatively mild stage of decline, while others even return to normal.
Dementia is a broad category of brain diseases that is diagnosed when memory loss and related symptoms affect the person’s ability to function on a day-to-day basis and is progressive. Only about 3% of 65-74 year-old people develop dementia, only 20% of 75-84 year old’s and 30%-50% of those over 85 years of age will develop the disease. The brain can produce new brain cells at any age, so significant memory loss is not an inevitable result of aging. Your lifestyle, health habits, and daily activities have a huge impact on the health of your brain.
Common types of dementia include Vascular Dementia (25%), which is caused by problems in the supply of blood to the brain, typically a series of minor strokes. Lewy Body Dementia (15%), involves a buildup of small clumps in the brain’s neurons and is a neurodegenerative disorder. Frontotemporal Dementia (10%) is evidenced by the progressive loss of the frontal/temporal lobes of the brain and is responsible for many young-onset dementia cases. Other types include Normal Pressure Hydrocephalus, caused by expansion of the cerebral ventricles, Parkinson’s disease, a degenerative disorder of the central nervous system, Syphilis, a sexually transmitted infection, and Creutzfeldt–Jakob disease (CJD), a fatal brain disorder caused by infectious proton material in the brain.
However, the most common type of dementia is Alzheimer’s disease (AD), which makes up 50 – 70% of dementia cases. It is a chronic neurodegenerative disease that usually starts slowly and worsens over time. The cause of Alzheimer’s disease is poorly understood. About 70% of the risk is believed to be genetic involving many genes. Other risk factors include a history of head injuries, depression, or hypertension. The disease process is associated with Amyloid Plaques in the brain. A probable diagnosis is based on history from relatives and behavioral observations.

Advanced medical imaging with Computed Tomography (CT) or Magnetic Resonance Imaging (MRI), and with Single-Photon Emission Computed Tomography (SPECT) or Positron Emission Tomography (PET) can be used to help exclude other cerebral pathology or subtypes of dementia. Another test involves a spinal tap. APOE Genotyping is a risk factor test, because it indicates whether there is an increased risk of AD but is not specifically diagnostic of AD.
Alzheimer’s disease (AD) is not curable but Dr. Niyom did talk about ways that may help prevent AD and other types of dementia. For example, avoid Insulin Inducer Foods: sweets and carbohydrates which promote insulin resistance, causing brain atrophy and vascular plaque. A High Fiber Diet decreases insulin resistance. Avoid red meat (L-carnitine) that induces cytotoxic substances. Use extra-virgin olive oil, since studies show its use increases intelligence, decreases cell energy utilization and decreases Tau protein and Amyloid plaque in brain tissue. Regular low to moderate exercise, social engagement, intellectual stimulation and early diagnosis/treatment is also recommended.
When memory loss and related symptoms affect you or a loved-one to the point of not being able to function on a day-to-day basis and is progressive, seek medical help. Otherwise, Dr. Niyom said you should be fine.
Dr. Niyom received his M.D. in 1993 from Chiang Mai University. In 2000, he received his Diplomate from the Thai Board of Neurology, Thai Neurology Association, Royal College of Medicine. Since 2000, he has been a neurology consultant with BHP.
After the presentation, MC Roy Albiston brought everyone up to date on upcoming events. This was followed by the “Open Forum” portion of the meeting, where questions are asked and answered and comments made about expat living in Thailand.
For more information on the Club and their activities, visit www.pcec.club.
To view a video of member Ren Lexander’s interview with Dr. Niyom Pisitpipattana visit https://www.youtube.com/watch?v=lK6zBo5nAhE



{kind=link}